
Paracetamol overdose
Paracetamol is widely used for its analgesic/anti-pyretic effects. It is also common to see accidental paediatric ingestion, unintentional self-administered supratherapeutic ingestions or intentional self-poisoning in the Emergency Department. While paracetamol is safe in normal doses, it is hepatotoxic and potentially fatal in overdose. Fortunately, N-acetylcysteine (NAC) is a safe and effective antidote which if used correctly prevents serious hepatic injury after paracetamol overdose.
Updated guidelines for the management of paracetamol poisoning in Australia and New Zealand were released in December 2019. A Guideline Summary has also been published. The ECI have produced this page to give quick access to the important flow charts and tables used in the management of paracetamol overdose, including when and how to use NAC based on these updated guidelines.
For advice at any time about management of paracetamol ingestion contact Poisons Information Centre on 13 11 26.
Unchanged recommendations
- Patients who present early should be given activated charcoal
- Patients at risk of hepatotoxicity should receive intravenous (IV) acetylcysteine
- The paracetamol nomogram should be used to assess the need for treatment in immediate release paracetamol ingestions with a known time of ingestion
- Cases that require different management include modified release paracetamol overdoses, large or massive overdoses, accidental liquid paracetamol ingestion in children and repeated supratherapeutic ingestions
- All patients with intentional self-poisoning with paracetamol should have a serum paracetamol performed, regardless of reported ingested dose
- It is important to check the units of measurement when using paracetamol nomograms with many laboratories recently changing from μmol/L (right axis) to mg/L (left axis)
Key changes to practice in the updated guidelines
Acetylcysteine treatment
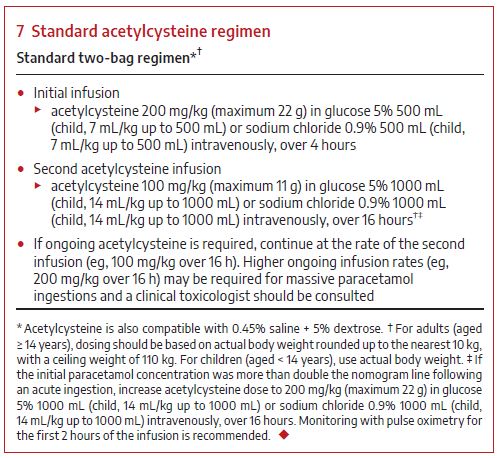
Standard treatment is now a two‐bag acetylcysteine IV infusion regime over 20 hours. This is just as effective as the previous three bag regime and significantly reduces adverse reactions. In some circumstances, a double dose regime is required.
Standard acetylcysteine treatment (use actual body weight):
Bag 1:
200 mg/kg (max 22 g) in 500 mL (glucose 5% or sodium chloride 0.9%) over 4 hours
For paediatrics use a dilution volume of 7mL/kg up to a max of 500 mL
Bag 2:
100 mg/kg (max 11 g) in 1000 mL (glucose 5% or sodium chloride 0.9%) over 16 hours
For paediatrics use a dilution volume of 14 mL/kg up to a max of 1000 mL
Double dose acetylcysteine treatment (use actual body weight):
Bag 1:
200 mg/kg (max 22 g) in 500 mL (glucose 5% or sodium chloride 0.9%) over 4 hours
For paediatrics use a dilution volume of 7mL/kg up to a max of 500 mL
Bag 2:
200 mg/kg (max 22 g) in 1000 mL (glucose 5% or sodium chloride 0.9%) over 16 hours
For paediatrics use a dilution volume of 14 mL/kg up to a max of 1000 mL
- Paracetamol ingestions between 10gm (200mg/kg) and 30gm (500mg/kg) should be treated with standard acetylcysteine infusion
- Massive paracetamol overdoses (over 30g) resulting in paracetamol concentrations more than double the nomogram line should be treated with double the dose of acetylcysteine (200 mg/kg) in the second bag of the treatment
- Paracetamol levels ≥ triple the nomogram line should be discussed with a clinical toxicologist as they may require higher acetylcysteine doses
Modified release paracetamol ingestion
- Modified release paracetamol ingestions of ≥ 10 g or ≥ 200 mg/kg (whichever is less) should receive a full course of acetylcysteine
- Modified release paracetamol ingestions of ≥ 30 g or ≥ 500 mg/kg should receive double the dose of acetylcysteine (200 mg/kg) in the second bag of the treatment
- All patients with intentional self-poisoning should have a serum paracetamol and ALT performed, regardless of reported ingested dose.
- It is important to check the units of measurement when using paracetamol nomograms. (Most laboratories now use mg/L rather than µmol/L)

Diagrams and Flowcharts
Paracetamol dosing that may be associated with acute liver injury (Box 1)
Paracetamol treatment nomogram (Rumack-Matthew nomogram) (Box 2)
Acute immediate release paracetamol ingestion management flow chart (Box 3)
Acute ingestion modified release paracetamol management flow chart (Box 4)
Repeated supratherapeutic ingestion management flow chart (Box 5)
Standard acetylcysteine regimen (Box 7)
{kind=link}
Criteria for cessation of ongoing treatment with acetylcysteine (Box 8)
{kind=link}
Paracetamol kinetics
Paracetamol is rapidly absorbed from the small intestine.
Peak serum concentrations occur within 2 hours for standard tablet or capsule formulations and 30 minutes for liquid preparations.
Twenty per cent of the ingested dose undergoes first-pass metabolism in the gut wall (sulphation).
Further elimination occurs by hepatic biotransformation.
About 90% is metabolised to inactive sulphate and glucuronide conjugates that are excreted in the urine.
Metabolism of the remainder is via cytochrome P450 and results in the highly reactive intermediary compound N-acetyl-p-benzoquinone imine (NAPQI).
With therapeutic paracetamol doses NAPQI is immediately bound by intracellular glutathione and eliminated in the urine as mercapturic adducts.
With increased paracetamol doses the increased NAPQI depletes glutathione stores and binds to other proteins, causing damage to the hepatocyte.
Management
Activated charcoal
Dose:
Activated charcoal (50 g for adult, 1 g/kg up to 50 g for children) if awake and co-operative.
Indications:
Immediate release paracetamol
- Within 2 hours of >10 g or >200 mg/kg (whichever is less)
- Within 4 hours of of ≥ 30 g
Modified release paracetamol
- Within 4 hours of ingestion of ≥ 10 g or ≥ 200 mg/kg (whichever is less) (includes mixed ingestion of immediate and modified release paracetamol)
- For massive overdoses (≥ 30 g or ≥ 500 mg/kg), absorption may continue up to 24 hours after ingestion; patients may benefit from activated charcoal beyond 4 hours
Acetylcysteine treatment
Threshold of treatment of paracetamol ingestion with acetylcysteine is shown in Box 1.
Dextrose (5%D) or Normal Saline (NS) may be used to make up acetylcysteine infusions.
Adults and Paediatrics
The acetylcysteine dose is the same for adults and paediatrics however the volume of infusion is adjusted in paediatric treatment to prevent fluid overload. (Box 7)
Standard IV acetylcysteine treatment (use actual body weight):
Bag 1: 200 mg/kg (max 22 g) in 500 mL (glucose 5% or sodium chloride 0.9%) over 4 hours
For paediatrics use a dilution volume of 7mL/kg up to a max of 500 mL
Bag 2: 100 mg/kg (max 11 g) in 1000 mL (glucose 5% or sodium chloride 0.9%) over 16 hours
For paediatrics use a dilution volume of 14 mL/kg up to a max of 1000 mL
Double dose IV acetylcysteine treatment (use actual body weight):
Bag 1: 200 mg/kg (max 22 g) in 500 mL (glucose 5% or sodium chloride 0.9%) over 4 hours
For paediatrics use a dilution volume of 7mL/kg up to a max of 500 mL
Bag 2: 200 mg/kg (max 22 g) in 1000 mL (glucose 5% or sodium chloride 0.9%) over 16 hours
For paediatrics use a dilution volume of 14 mL/kg up to a max of 1000 mL
Management of immediate release paracetamol ingestion
Single Dose
Single immediate release paracetamol ingestions with a known time of ingestion should be managed using the Acute immediate release paracetamol ingestion management flow chart (Box 3) in conjunction with the Paracetamol treatment nomogram (Rumack-Matthew nomogram) (Box 2).
If the result of a paracetamol level will be available within 8 hours of ingestion, then acetylcysteine may be delayed until the paracetamol level is available. The Acute immediate release paracetamol ingestion management flow chart for rural and remote facilities (no pathology availability) (Box 6) should be used to direct treatment in facilities without access to paracetamol level testing.
If the paracetamol level will not be available within 8 hours and the dose exceeds the threshold for toxicity (Box 1) or there are clinical signs of toxicity (nausea, vomiting, right upper quadrant pain or tenderness), acetylcysteine should be commenced and a decision made to continue or cease the infusion when a paracetamol level is available.
Multiple dose
- Excessive paracetamol taken for therapeutic purposes should be managed using the Repeated supratherapeutic ingestion management flow chart (Box 5)
- Ingestions taken for purpose of self-harm over a period of more than 2 hours should be treated as per the Acute immediate release paracetamol ingestion management flow chart (Box 3) using the earliest time of ingestion for the Paracetamol treatment nomogram (Rumack-Matthew nomogram) (Box 2)
- If it is more than 8 hours since the first dose of paracetamol or the paracetamol concentration cannot be obtained within 8 hours, then commence treatment with acetylcysteine.
If the first paracetamol concentration was measured within 2 hours of the last ingested paracetamol dose, it should be repeated after 2 hours to ensure there is no ongoing absorption. If either concentration is above the nomogram line (using time from the earliest ingestion), start or continue treatment with acetylcysteine.
A paracetamol level and ALT should be taken 4 hours after the last known paracetamol ingestion.
Pediatric liquid paracetamol ingestion
In children under 6 years who have ingested > 200 mg/kg, a serum paracetamol level should be taken at least 2 hours after the time of ingestion.
If the 2–4-hour concentration is below 150 mg/L (1000 μmol/L), acetylcysteine is not required.
If the 2-hour paracetamol concentration is greater than 150 mg/L (1000 μmol/L), this should be repeated 4 hours after ingestion and acetylcysteine commenced if this is 150 mg/L or more (1000 μmol/L).
A 2-hour concentration should only be used in a well child under 6 years of age with isolated liquid paracetamol ingestion. In all other cases, a 4-hour concentration should be performed.
Further, for children who present later than 4 hours after ingestion or in children older than 6 years of age, treatment is as per the adult acute paracetamol exposure guideline.
Management of modified release paracetamol
The management of modified release paracetamol ingestions is shown in Acute ingestion modified release paracetamol management flow chart (Box 4).
ALT and a paracetamol level should be taken two hours before the end of the second bag.
Acetylcysteine should be continued if ALT is elevated (> 50 U/L) and increasing (if baseline ALT > 50 U/L) or if the paracetamol concentration is 10 mg/L or over (66 μmol/L).
Higher doses of acetylcysteine may be required in subsequent infusions if the paracetamol concentration remains 100 mg/L or over (> 660 μmol/L) and further advice should be sought.
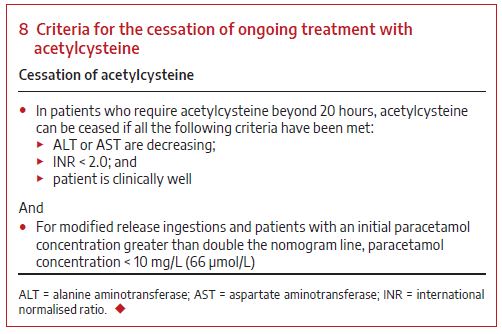
Ceasing acetylcysteine infusion
In those patients requiring extended treatment, the Criteria for the cessation of ongoing treatment with acetylcysteine are shown in Box 8.
The infusion can be ceased if all the following criteria are met:
- ALT or AST are decreasing;
- INR < 2.0; and
- Person is clinically well
AND
- For infusions started for modified release ingestions and for those with an initial paracetamol level greater than double the nomogram line, the paracetamol concentration is < 10 mg/L (66 µmol/L).
Liver transplant unit referral
A liver transplant unit should be consulted if any of the following criteria are met:
- INR greater than 3.0 at 48 hours or greater than 4.5 at any time
- oliguria or creatinine greater than 200 µmol/L
- persistent acidosis (pH < 7.3) or arterial lactate greater than 3 mmol/L
- systolic hypotension with blood pressure below 80 mmHg, despite resuscitation
- hypoglycaemia, severe thrombocytopenia or encephalopathy of any degree, or
- any alteration of consciousness (Glasgow Coma Score < 15) not associated with sedative co-ingestions.
Do not give clotting factors unless the patient is bleeding or after discussion with a liver transplant unit.
Situations where advice should be sought from a Poisons Information Centre
Poisons Information Centre should be contacted for advice on 13 11 26 for:
- very large overdoses — immediate release or modified release paracetamol overdoses of 50 g or over or 1 g/kg (whichever is less)
- high paracetamol concentrations of more than triple the nomogram line
- intravenous paracetamol errors or overdoses (as the treatment threshold is lower)
- patients with hepatotoxicity (ALT > 1000 IU/L)
- neonatal paracetamol poisonings